
Related topic: This article is part of The Foundational Longevity Stack. If you want the broader overview, start with Foundational Longevity Stack: Evidence-Based Core Supplements. The pursuit of healthy aging has shifted from vague wellness aspirations to precision-targeted interventions backed by molecular science. Among the most promising—and debated—strategies is the combined use of vitamin D3 and K2 for longevity support.
This guide provides a structured framework for healthcare providers, clinicians, and informed patients seeking to optimize lifespan through targeted nutrient interventions. The primary audience includes primary care physicians, endocrinologists, geriatric specialists, and health-conscious adults over 50 looking for evidence-based strategies to slow age-related decline.
Several key controversies shape this landscape. Debates persist over optimal serum 25(OH)D thresholds for defining vitamin d deficiency. Questions remain about whether vitamin K2 MK-7 truly outperforms other forms like MK-4. And while telomere preservation data from major trials looks promising, cardiovascular benefits from vitamin d supplementation remain inconsistent across studies.
The practical goals here are clear: establish safe supplementation protocols, enable proper risk stratification, and implement monitoring strategies that prevent complications like hypercalcemia or misdirected calcium deposits in soft tissues.
The body’s regulatory mechanisms play a crucial role in maintaining calcium balance, and dysfunction in these mechanisms can contribute to age-related complications such as arterial calcification.
Let’s break down what the evidence actually shows.
Background: Vitamin D Basics
Understanding vitamin d at the molecular level is essential before diving into longevity applications. This hormone-like nutrient exists in two primary chemical forms, undergoes a two-step activation process, and ultimately controls calcium absorption in ways that affect nearly every organ system.
In addition to its role in calcium metabolism, vitamin D also influences cell growth by modulating cellular proliferation, differentiation, and apoptosis, which are important for tissue maintenance and overall health.
Chemical Forms and Nomenclature
Vitamin D comes in two major forms:
| Form | Name | Source | Relative Potency |
|---|---|---|---|
| D2 | Ergocalciferol | Plant-derived (UV-exposed yeast/fungi) | Baseline |
| D3 | Cholecalciferol | Animal-derived or synthesized in human skin | 1.7-2x more potent |
Cholecalciferol (D3) demonstrates approximately 1.7 to 2 times greater potency in raising serum 25(OH)D levels compared to ergocalciferol. This difference stems from D3’s higher binding affinity to the vitamin D binding protein in circulation.
When UVB radiation (280-315 nm wavelength) strikes the skin, it converts 7-dehydrocholesterol into pre-vitamin D3, which then isomerizes to cholecalciferol. This is why sun exposure remains the most efficient natural source of vitamin D for most healthy individuals.
Hepatic Activation
The liver performs the first activation step. Here, cholecalciferol is hydroxylated by the enzyme 25-hydroxylase (primarily CYP2R1) to form 25-hydroxyvitamin D, written as 25(OH)D.
This metabolite is the major circulating form of vitamin D and serves as the standard biomarker for assessing vitamin d status. With a half-life of 2-3 weeks, 25(OH)D reflects long-term intake rather than moment-to-moment fluctuations.
When your lab orders a “vitamin D level,” they’re measuring 25(OH)D.
Renal Activation to the Active Form
The kidneys handle the second activation step. Here, 25(OH)D is further hydroxylated by 1-alpha-hydroxylase (CYP27B1) to produce 1,25-dihydroxyvitamin D—also called calcitriol or 1,25(OH)2D.
Calcitriol is the biologically active hormone that binds the vitamin D receptor (VDR) to exert genomic effects throughout the body. This conversion is tightly regulated by:
- Parathyroid hormone (PTH)
- Serum calcium levels
- Serum phosphate levels
Beyond the kidneys, extrarenal production of calcitriol occurs in immune cells, skin, and other tissues for local (paracrine) functions. This helps explain vitamin D’s role in immune function beyond traditional calcium homeostasis.
Role in Calcium Uptake
Calcitriol’s most well-established function involves enhancing calcium uptake in the gut. The active hormone induces expression of several specific proteins in duodenal enterocytes:
- TRPV6: Transient receptor potential vanilloid 6 calcium channels
- Calbindin-D9k: Intracellular calcium binding proteins
- PMCA1b: Plasma membrane calcium ATPase on the basolateral membrane
Together, these proteins increase active transcellular absorption by up to 30-40% in individuals with vitamin d insufficiency or deficiency. Passive process absorption through paracellular diffusion also occurs but contributes less to overall calcium absorption efficiency.

Vitamin D3 and K2 Mechanisms Related to Longevity
The longevity rationale for combining D3 with K2 centers on a fundamental problem: vitamin D enhances calcium absorption, but without K2, that extra calcium may deposit in the wrong places. When calcium is misdirected, plaque accumulates in the arteries, contributing to atherosclerosis and increasing cardiovascular risk.
K2 Role in Directing Calcium Transport
Vitamin K2, particularly the menaquinone-7 (MK-7) form, activates two proteins critical for proper calcium distribution:
- Matrix Gla Protein (MGP): When activated (carboxylated), MGP inhibits vascular calcification by binding and sequestering calcium in soft tissues
- Osteocalcin: When carboxylated, osteocalcin promotes hydroxyapatite crystal formation in bone matrix
The activation process involves gamma-carboxylation by the enzyme gamma-glutamyl carboxylase, using reduced vitamin K (KH2) as a cofactor. This is why adequate K2 intake is essential for directing calcium ions toward bones and away from arterial walls.
MK-7 has a half-life of approximately 3 days, compared to just 1 hour for MK-4. This longer half-life translates to more consistent tissue concentrations and potentially greater effectiveness at typical supplemental doses.
Enhanced Calcium Uptake from D3
Vitamin D3 synergistically boosts intestinal calcium absorption via VDR-mediated pathways. In individuals with deficient vitamin d levels, supplementation can potentially elevate circulating calcium by 10-20%.
This increase in calcium influx is beneficial for preventing osteoporosis but creates a potential problem: where does all that extra calcium go?
Without adequate vitamin K2 to activate the proteins that direct calcium transport, the risk of ectopic calcification—particularly in blood vessels—may increase.
K2 and Vascular Calcium Deposits
Data from the Rotterdam Study provides compelling observational evidence for K2’s protective effects. Higher dietary K2 intake (above 32 mcg/day) was associated with:
- 57% reduced risk of aortic calcification
- 26% lower all-cause mortality over 7-10 years
- Up to 12% reduction in arterial stiffness measures
These findings suggest K2 plays a crucial role in preventing calcium deposits from accumulating in arterial elasticity-compromising locations.
Implications for Bone Health
The D3-K2 synergy extends to skeletal outcomes. Meta-analyses of combined supplementation in postmenopausal women show:
- 1-2% annual improvement in bone mineral density
- 20-30% reduction in fracture risk
- Decreased bone resorption markers like CTX
These benefits emerge through enhanced osteocalcin activity—K2 carboxylates osteocalcin, making it capable of binding calcium to bone matrix, while D3 provides the raw material by increasing calcium absorption.
Calcium Transport and Coronary Artery Calcification
Understanding the connection between calcium metabolism and arterial disease is essential for appreciating why the D3-K2 combination matters for cardiovascular health. High cholesterol is a major modifiable risk factor for arterial calcification and should be managed alongside vitamin D3 and K2 interventions.
Defining Coronary Artery Calcification
Coronary artery calcification (CAC) represents the pathological deposition of calcium phosphite crystals in the intimal layer of coronary arteries. Clinicians quantify this using CT imaging and the Agatston scoring system:
| CAC Score | Risk Category |
|---|---|
| 0 | Very low risk |
| 1-99 | Low to moderate |
| 100-399 | Moderate risk |
| >400 | High risk |
Coronary artery calcium scoring serves as an independent predictor of myocardial infarction, with hazard ratios ranging from 2.5 to 10-fold increased risk per unit increase in score category. Elevated CAC scores are strongly associated with an increased risk of heart attack, highlighting the importance of early detection and prevention.
How Calcium Transport Affects Arterial Calcification
Dysregulated calcium transport—particularly when amplified by D3-induced hyperabsorption without adequate K2 carboxylation of MGP—promotes a dangerous cellular transformation.
Vascular smooth muscle cells can undergo “osteogenic transdifferentiation,” essentially transforming into osteoblast-like cells that express:
- Runx2 (a transcription factor for bone formation)
- BMP-2 (bone morphogenetic protein 2)
These transformed smooth muscle cells create microcalcifications that eventually coalesce into larger calcium deposits. The process is particularly accelerated in:
- Chronic kidney disease (CKD)
- Diabetes mellitus
- States where fetuin-A and pyrophosphate inhibitors are deficient
Mechanistic Rationale for K2 Reducing Calcification
Carboxylated MGP (cMGP) directly suppresses BMP-2 signaling and reduces vascular smooth muscle cell apoptosis—two key drivers of arterial calcification.
Clinical evidence supports this mechanism. The INTRICATE study demonstrated that 180 mcg MK-7 daily achieved:
- 6-8% reduction in carotid-femoral pulse wave velocity (cfPWV)
- 12% slower CAC progression over 2 years in CKD patients
Factorial trial designs confirm additive effects when K2 is combined with D3, supporting the synergy hypothesis for prevention strategies targeting vascular calcification.
Cardiovascular Outcomes and Heart Health
Moving from mechanisms to outcomes, what does the clinical evidence actually show for D3 and K2 effects on cardiovascular risk?
In cases of severe coronary artery calcification or blockage, percutaneous coronary intervention (PCI) may be required to restore blood flow and reduce the risk of major cardiac events.
Observational Links Between Vitamin D and Heart Health
Large cohort studies consistently associate low 25(OH)D levels with adverse cardiovascular outcomes. Data from the national health and nutrition examination survey (NHANES) and Framingham cohorts link vitamin d deficiency (< 20 ng/mL) to:
- 1.5 to 2-fold higher cardiovascular mortality
- Increased risk of hypertension
- Higher incidence of metabolic syndrome
However, a U-shaped relationship appears at higher levels, with potential risks emerging above 50 ng/mL. This finding has important implications for supplementation targets.
Mendelian randomization studies temper causal interpretations—the association may not reflect direct causation.
Trials on Vitamin D3, K2, and Coronary Artery Calcification
The largest vitamin D trial to date, VITAL, enrolled 25,871 adults who received 2000 IU D3 daily for 5.3 years. Key findings included:
- No overall reduction in major cardiovascular events
- 28% lower autoimmune disease incidence
- Telomere preservation equivalent to 3 years less cellular aging
The telomere finding deserves attention. In a 1054-participant substudy, D3 supplementation resulted in 140 fewer base pairs lost over 4 years compared to placebo—a marker of slowed cellular health decline (Br J Nutr et al data).
For combined D3-K2 interventions, a 24-week randomized trial in 151 long-COVID patients (2000 IU D3 + 240 mcg MK-7) showed:
- 20-30% reduction in CRP (inflammatory marker)
- 15% decrease in oxidized low density lipoprotein
- 40% improvement in symptoms like chest pain and body pain
These findings suggest cardiovascular protection may occur through anti-inflammatory and anti-calcific pathways rather than direct lipid modification.
Evidence for Vitamin D Effects on Blood Pressure
Meta-analyses of 46 randomized trials show modest effects of vitamin d supplements on blood pressure:
- 2-4 mmHg systolic reduction in deficient hypertensives
- Non-significant effects in those with adequate vitamin d levels
For patients with high blood pressure and concurrent deficiency, correcting vitamin d status may provide adjunctive benefit. However, vitamin D alone should not be considered primary antihypertensive therapy.
Imaging and Scoring Triggers for Cardiac Risk Assessment
Consider coronary artery calcium scoring via CT for patients meeting any of these criteria:
- 10-year ASCVD risk >7.5%
- Family history of premature coronary artery disease
- 25(OH)D levels < 30 ng/mL with other risk factors
- Intermediate risk requiring treatment decision clarification
CAC scoring helps identify patients who may benefit most from aggressive prevention strategies, including optimized D3-K2 supplementation protocols.

Metabolic Effects Including Diabetes Mellitus
Beyond cardiovascular health, vitamin D influences metabolic function through direct effects on insulin sensitivity and glucose regulation.
Vitamin D Effects on Insulin Sensitivity
Vitamin D enhances insulin sensitivity through VDR upregulation of several key signaling molecules:
- PPAR-gamma in adipocytes
- IRS-1/2 (insulin receptor substrate) in adipocytes and myocytes
- GLUT4 translocation for glucose uptake
These molecular mechanisms translate to reduced hepatic gluconeogenesis and improved peripheral glucose disposal. Meta-analyses consistently link vitamin d deficiency (< 20 ng/mL) to 1.5 to 2-fold increased risk of type 2 diabetes mellitus.
Randomized Trials on Diabetes Prevention
Several large trials have examined vitamin D for diabetes prevention:
| Trial | Participants | Intervention | Key Finding |
|---|---|---|---|
| PREDIMED | 1301 high-risk adults | Vitamin D (various doses) | 15% relative risk reduction |
| D2d | 2423 prediabetics | 4000 IU D3 daily | 15% reduced diabetes incidence |
| VITAL | 25,871 general adults | 2000 IU D3 daily | No significant effect |
The D2d trial specifically targeted individuals with prediabetes, showing meaningful benefit over 2.5-5 years. The VITAL trial’s null finding may reflect the lower-risk population studied.
These results suggest that diabetes mellitus prevention strategies incorporating vitamin D work best in high-risk populations with documented deficiency.
Monitoring Glycemic Markers During Supplementation
For diabetic patients receiving vitamin d supplements, implement the following monitoring protocol:
- Check HbA1c and fasting glucose quarterly
- Target 25(OH)D levels of 40-60 ng/mL
- Watch for transient glucose elevations (5-10 mg/dL) with hypervitaminosis
Excessive 1,25(OH)2D can paradoxically suppress insulin secretion, underscoring the importance of avoiding over-supplementation in metabolically vulnerable patients.
Vitamin D Deficiency: Screening and Assessment
Proper identification of deficiency is foundational to any supplementation strategy. However, defining “deficiency” remains surprisingly contentious.
Thresholds and Controversies
The Endocrine Society defines vitamin d deficiency as serum 25(OH)D:
- < 12 ng/mL: Severe deficiency
- < 20 ng/mL: Deficiency
- 21-29 ng/mL: Insufficiency
- 30-50 ng/mL: Optimal for extraskeletal benefits (controversial)
The Institute of Medicine (IOM) takes a more conservative stance, considering 20 ng/mL sufficient for bone health in most healthy adults.
This discrepancy creates clinical uncertainty. Should we treat a patient with 25 ng/mL? The answer depends on your goals—skeletal maintenance versus optimization of immune responses, cardiovascular function, and longevity markers.
Harmonized laboratory assays have reduced interlab variability by 10-20%, improving comparability across testing facilities.
When to Test Serum 25(OH)D Levels
Screen the following at-risk groups:
- Age >65 years
- BMI >30
- Dark skin pigmentation
- Limited sun exposure (indoor workers, institutionalized, northern latitudes)
- Malabsorption syndromes (IBD, celiac, post-bariatric)
- Osteoporosis or fragility fractures
- Chronic kidney disease
- Medications affecting vitamin D metabolism (anticonvulsants, glucocorticoids)
Test timing matters. Late winter measurements capture trough levels and reveal true deficiency status better than summer testing.
Healthcare Provider Role in Interpreting Results
A single 25(OH)D level tells an incomplete story. Your healthcare provider should interpret results alongside:
- PTH levels: Elevated PTH (>65 pg/mL) signals functional deficiency even with borderline 25(OH)D
- Serum calcium: Rules out hypercalcemia before aggressive supplementation
- eGFR: Renal function affects activation to calcitriol
- Albumin: For correcting total calcium measurements
This comprehensive assessment prevents both under-treatment of true deficiency and inappropriate supplementation in contraindicated conditions.
Sources, Sun Exposure, and Bioavailability
Before reaching for supplements, understanding natural sources and factors affecting bioavailability provides context for proper management of vitamin d status.
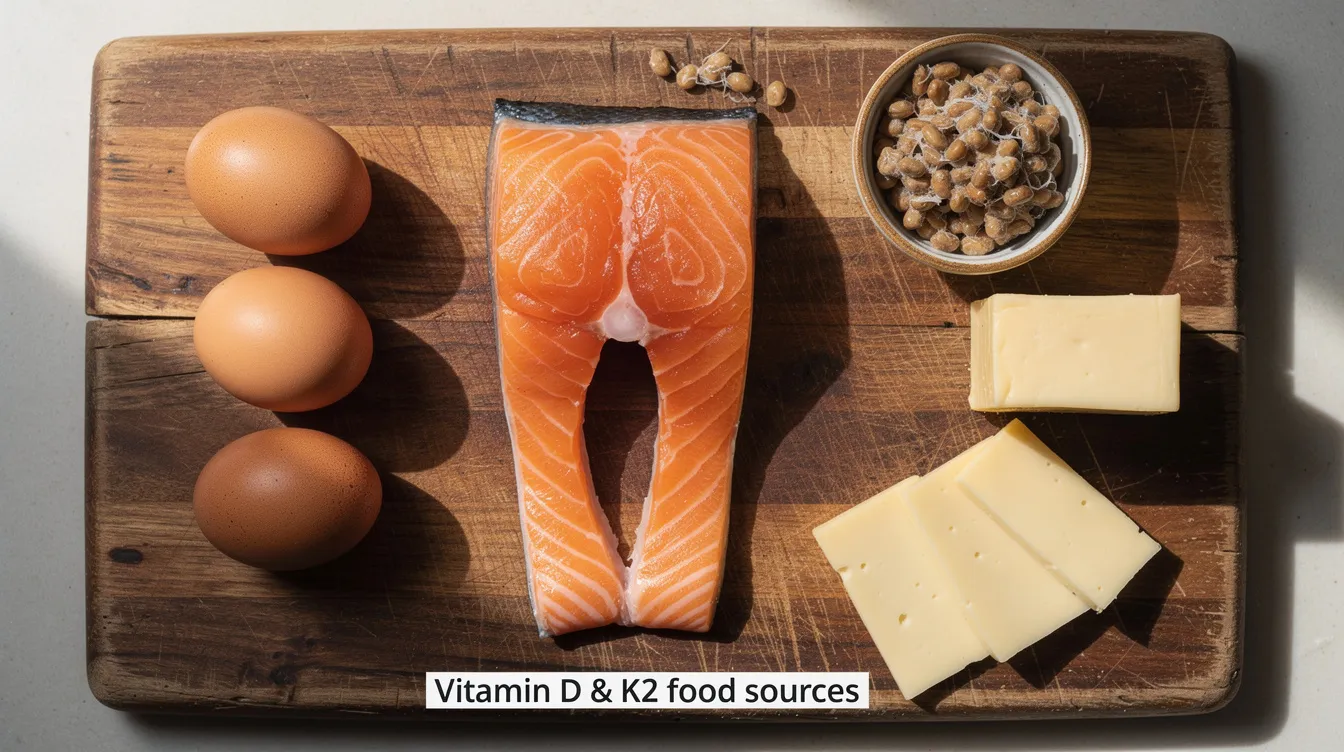
Dietary Sources of Vitamin D3 and K2
Vitamin D occurs naturally in few foods, making dietary sufficiency challenging for many:
Vitamin D3 Sources: | Food | Approximate Content | |——|———————| | Wild salmon (3 oz) | 600-1000 IU | | Cod liver oil (1 tsp) | 400-1000 IU | | Egg yolks (1 large) | 40 IU | | Fortified milk (1 cup) | 100-120 IU |
Vitamin K2 Sources: | Food | Approximate Content | |——|———————| | Natto (50g) | 1100 mcg MK-7 | | Goose liver (100g) | 370 mcg | | Hard cheeses (100g) | 50-75 mcg | | Grass-fed butter | Variable MK-4 |
For most people eating Western diets, achieving adequate K2 intake from food alone requires deliberate inclusion of fermented foods or organ meats.
Safe Sun Exposure Guidance
UVB radiation (280-315 nm) enables endogenous vitamin D synthesis. Guidelines for safe sun exposure:
- Duration: 10-30 minutes midday exposure
- Frequency: 2-3 times weekly
- Skin area: Full-body or substantial (arms, legs, face)
- Expected yield: 10,000-25,000 IU in light-skinned individuals
Those with dark skin require 1.5-3 times longer exposure to achieve equivalent synthesis due to melanin’s UV-filtering effect.
By age 70, cutaneous 7-dehydrocholesterol decreases by approximately 50%, reducing synthetic capacity even with adequate sun exposure.
Factors That Reduce Oral Absorption
Several conditions and other factors impair vitamin D bioavailability:
- Bile acid malabsorption: IBD, post-cholecystectomy, gastric bypass surgery
- Obesity: Hydrophobic sequestration in adipose tissue (adjust dose by +0.75 mcg/kg above normal BMI)
- Polyphenol interactions: Some plant compounds inhibit CYP enzymes
- Concurrent medications: Cholestyramine, orlistat, mineral oil
- Age-related changes: Reduced absorptive surface area
Fat-soluble vitamin D requires dietary fat for absorption—taking supplements with meals significantly improves bioavailability.
Food-First Strategies
Before recommending supplementation, optimize dietary intake:
- Target 3 servings fatty fish weekly
- Include fermented soy (natto) or aged cheeses regularly
- Use cod liver oil as a concentrated source
- Choose fortified dairy or plant milks
This food-first approach can achieve 20-50% of recommended intake, reducing supplementation requirements and providing complementary nutrients.
Supplementation Strategies for Longevity
When diet and sun exposure prove insufficient, targeted supplementation becomes necessary. The following protocols reflect current evidence for longevity optimization.
Dosing Ranges for Vitamin D3 by Risk Group
Vitamin D3 dosing should be individualized based on baseline status and risk factors:
| Risk Category | Starting Dose | Target 25(OH)D |
|---|---|---|
| General healthy adults | 1000-2000 IU daily | 30-50 ng/mL |
| Deficient (< 20 ng/mL) | 2000-4000 IU daily | 40-60 ng/mL |
| Obese (BMI >30) | 3000-4000 IU daily | 40-60 ng/mL |
| Malabsorption syndromes | 4000-6000 IU daily | Monitor closely |
| Post-bariatric | Individualized | Monitor closely |
The VITAL trial used 2000 IU daily and achieved measurable benefits on telomere preservation and autoimmune disease incidence rate reduction. This dose represents a reasonable starting point for most adults seeking longevity benefits.
Dosing Guidance for Vitamin K2 Forms
MK-7 is the preferred K2 form due to its superior pharmacokinetics:
- Maintenance dose: 100-180 mcg MK-7 daily
- Higher risk/active supplementation: 180-360 mcg MK-7 daily
- Long-COVID protocol dose: 240 mcg MK-7 (from published trial)
MK-4 requires substantially higher doses (15 mg) to achieve therapeutic tissue levels due to its 1-hour half-life versus MK-7’s 3-day half-life. For most applications, MK-7 offers better convenience and consistency.
Co-Administration Rationale
Combining D3 with K2 addresses the fundamental calcium direction problem. A practical ratio of 1000 IU D3 to 100 mcg K2 provides:
- Adequate calcium absorption enhancement
- Sufficient K2 to activate MGP and osteocalcin
- Prevention of soft-tissue calcification risk
Studies suggest that D3 supplementation alone may increase CAC scores by 10-15% in some populations without concurrent K2. This finding strongly supports the synergistic approach.
Preferred Formulations and Timing
Optimize absorption and effectiveness through formulation and timing choices:
Formulation preferences:
- Liposomal forms: 2-3x improved bioavailability
- MCT oil-based softgels: Enhanced fat-soluble absorption
- Combination D3/K2 products: Convenience and compliance
Timing considerations:
- Take with fat-containing meals (essential for absorption)
- Evening dosing may mimic circadian patterns
- Consistency matters more than specific timing
- Avoid concurrent high-dose calcium supplements (space by 2-3 hours)
Safety, Interactions, and Monitoring
Like any intervention affecting calcium metabolism, D3-K2 supplementation requires appropriate safety monitoring.
Hypercalcemia Risk Factors
Elevated calcium risk increases with:
- 25(OH)D levels >100 ng/mL
- Doses exceeding 10,000 IU daily (chronic)
- Primary hyperparathyroidism
- Granulomatous diseases (sarcoidosis, tuberculosis)
- Concurrent thiazide diuretics
- Lithium therapy
- Lymphoma
Patients with these risk factors require closer monitoring and potentially lower supplementation thresholds.
Hypercalcemia Symptoms
Educate patients to recognize warning signs:
- Fatigue and weakness
- Nausea and vomiting
- Constipation
- Polyuria and polydipsia
- Confusion or cognitive changes
- Bone pain
- ECG changes (shortened QT interval)
Early recognition prevents progression to more severe manifestations including renal failure and cardiac arrhythmias.
When to Measure Serum Calcium
Monitoring recommendations based on dose and risk:
| Scenario | Calcium Monitoring Frequency |
|---|---|
| Low-dose (< 2000 IU) + low risk | Baseline, then annual |
| Moderate dose (2000-4000 IU) | 3 months, then every 6-12 months |
| High dose (>4000 IU) | 3 months, then every 6 months |
| High-risk patients | 3 months, then every 3-6 months |
Measure both total calcium (concerning if >10.5 mg/dL) and consider ionized calcium (>1.35 mmol/L) for ambiguous cases or hypoalbuminemia.
Interactions with Anticoagulant Medications
K2 supplementation has important drug interactions:
Vitamin K antagonists (warfarin):
- K2 competes for vitamin K epoxide reductase
- Can reduce anticoagulation effect
- Requires INR monitoring with any K2 supplementation
- Dose adjustments may be necessary
Direct oral anticoagulants (DOACs):
- No significant interaction
- K2 supplementation generally safe
- Standard dosing appropriate
Always review anticoagulation status before recommending K2 supplementation.
Upper Intake Limits for Vitamin D
Established safety thresholds:
- IOM upper limit: 4000 IU daily (general population)
- Endocrine Society: Up to 10,000 IU may be safe short-term
- Toxicity threshold: Generally 25(OH)D >150 ng/mL
The national institutes of health and blood institute recommendations emphasize individual assessment over rigid population limits.
Signs of Vitamin D Toxicity
Frank toxicity typically requires:
- 25(OH)D levels >150 ng/mL
- Prolonged high-dose intake (>50,000 IU weekly for months)
Manifestations include severe hypercalcemia, nephrocalcinosis, renal failure, and cardiac arrhythmias. This degree of toxicity is rare with typical supplementation protocols but has occurred with manufacturing errors or extreme self-supplementation.
Practical Clinical Pathway for Healthcare Provider
Implementing D3-K2 supplementation requires systematic assessment and follow-up. The following pathway standardizes care delivery.
Checklist for Initial Patient Assessment
Complete before initiating supplementation:
Laboratory testing:
- Serum 25(OH)D
- PTH (intact)
- Calcium (total and/or ionized)
- Albumin
- Creatinine/eGFR
- Lipid panel (high density lipoprotein, LDL, triglycerides)
- HbA1c
- Consider CAC score if cardiovascular risk factors present
Clinical assessment:
- Current medications (especially anticoagulants, thiazides)
- Supplement inventory (including calcium, other fat-soluble vitamins)
- Diet history (fatty fish, fermented foods, fortified products)
- Sun exposure patterns
- History of kidney stones, sarcoidosis, malabsorption
- Family history of hypercalcemia or parathyroid disease
Follow-Up Testing Intervals by Risk Category
Low-risk patients (replete sun-exposed, no comorbidities):
- Recheck 25(OH)D in 12 months
- Annual monitoring thereafter if stable
High-risk patients (deficient + CVD/DM/malabsorption):
- Recheck 25(OH)D at 3 months
- Repeat at 6 months
- Transition to every 6-12 months once stable
- Include calcium/PTH at each visit
Special populations (CKD, post-bariatric, granulomatous disease):
- Individualized monitoring every 3 months initially
- Consider specialty co-management
Documentation Items for Shared Decision-Making
Ensure medical records include:
- Baseline lab values and interpretation
- Specific supplementation goals (target 25(OH)D range)
- Dose rationale with literature support
- Discussion of U-curve risks at high levels
- Patient understanding of monitoring requirements
- Informed consent for off-label high-dose protocols
- Follow-up plan with contingencies
Referral Triggers to Specialists
Consider specialty consultation for:
- Abnormal PTH or calcium at baseline
- CAC score >300 Agatston units
- Failure to achieve target 25(OH)D despite adequate dosing
- Suspected malabsorption requiring evaluation
- Complex drug interactions
- Pregnancy (refer to obstetric care for pregnant women)
- Suspected granulomatous disease
Endocrinology, cardiology, and gastroenterology may all contribute to complex cases.
Research Gaps and Future Directions
Despite promising mechanistic and observational data, significant evidence gaps remain for D3-K2 longevity applications.
Lack of Longevity-Focused Randomized Trials
No randomized controlled trials exceeding 10 years have examined D3-K2 combinations with longevity endpoints. Current evidence limitations include:
- Most trials focus on single outcomes (fractures, cardiovascular events)
- Combination D3-K2 trials remain small and short-term
- Telomere data from VITAL is promising but represents a proxy endpoint
- Few studies specifically enroll populations >65 years
Further research with extended follow-up and composite longevity outcomes is essential.
Proposed Studies on Vitamin D3, K2, and Coronary Calcification
A phase III trial design to address key gaps:
Population: Adults 65+ with baseline CAC scores 100-400
Intervention: D3 2000 IU + K2 240 mcg daily vs. placebo
Primary endpoints:
- CAC progression (annual CT)
- Telomere attrition rate
- Composite cardiovascular events
- All-cause mortality
Duration: 5-10 years
Target enrollment: 3000-5000 participants for adequate power
Standardized Endpoints and Assay Harmonization
Methodological improvements needed:
- 25(OH)D measurement standardization via LC-MS/MS (target CV < 10%)
- Harmonized telomere length qPCR protocols
- Consensus CAC scoring methodology
- Validated composite longevity endpoints
- Standardized K2 status biomarkers (undercarboxylated osteocalcin ratios)
Without these standardizations, meta analysis across trials remains challenging and conclusions uncertain.
Practical Takeaways and Communication Points
Translating evidence into practice requires clear, actionable guidance for both clinicians and patients.
Clinician Action Items
Screening and assessment:
- Screen at-risk populations annually for vitamin D deficiency
- Include PTH and calcium with 25(OH)D testing
- Consider CAC scoring for intermediate cardiovascular risk patients
Treatment approach:
- Target 25(OH)D of 40-60 ng/mL for longevity optimization
- Add K2 (180-240 mcg MK-7) when D3 doses exceed 2000 IU
- Use combination formulations when possible for compliance
Monitoring:
- Check calcium and PTH every 6 months during active titration
- Annual monitoring once stable
- Document shared decision-making and goals
Concise Advice for Patients
Key messages for patient communication:
- “Take 2000 IU vitamin D3 plus 180 mcg vitamin K2 (MK-7) daily with a meal containing fat”
- “Get 15 minutes of midday sun exposure 3 times weekly when possible”
- “Eat fatty fish 2-3 times per week”
- “Get your vitamin D level tested yearly”
- “Report symptoms like nausea, excessive thirst, or confusion”
Quick Reference Dosing Table
| Risk Level | Vitamin D3 | Vitamin K2 (MK-7) | Monitoring |
|---|---|---|---|
| Low-risk (healthy, sun-exposed) | 1000 IU daily | 100 mcg daily | Annual |
| Moderate (age >65, limited sun) | 2000 IU daily | 180 mcg daily | Every 6-12 months |
| High-risk (deficient, CVD/DM) | 2000-4000 IU daily | 180-240 mcg daily | Every 3-6 months |
| Maximum | 4000 IU daily (routine) | 360 mcg daily | Per protocol |
Special considerations:
- Obese patients: Add +0.75 mcg/kg above normal BMI
- Post-gastric bypass surgery: Individualized dosing, close monitoring
- Warfarin users: Coordinate K2 with anticoagulation clinic
- Heavy metals exposure or environmental concerns: Standard protocols apply
Key Takeaways
The vitamin D3 and K2 synergy for longevity rests on solid mechanistic foundations:
- Vitamin D3 enhances calcium absorption, immune function, and cellular function through VDR-mediated pathways
- Vitamin K2 (particularly MK-7) directs calcium toward bones and away from arteries via MGP and osteocalcin activation
- Combined supplementation addresses the fundamental calcium distribution challenge
- VITAL trial data shows telomere preservation equivalent to 3 years less aging with 2000 IU D3
- D3-K2 combinations reduce inflammatory markers and may slow coronary artery calcification progression
Current evidence supports:
- Screening at-risk populations for vitamin d deficiency
- Targeting 40-60 ng/mL 25(OH)D for extraskeletal and longevity benefits
- Adding K2 when D3 supplementation exceeds 2000 IU daily
- Regular monitoring of calcium, PTH, and vitamin d levels
Gaps remain:
- No large-scale, long-term RCTs with combined D3-K2 and longevity endpoints
- Optimal thresholds remain debated
- Individual response variability is substantial
Conclusion
The evidence for vitamin D3 and K2 as a longevity intervention continues to strengthen, though definitive proof awaits larger, longer trials. What we know suggests meaningful benefits for bone mineral density, cardiovascular health, metabolic function, and potentially cellular aging markers.
For clinicians, the path forward involves systematic screening, individualized dosing, appropriate co-administration of K2 with D3, and regular monitoring to ensure safety and effectiveness. For patients, a combination of dietary optimization, sensible sun exposure, and targeted supplementation offers a practical approach to supporting overall health across the lifespan.
Work with your healthcare provider to establish baseline testing, implement an appropriate protocol, and monitor your health status over time. The science continues to evolve, but the current evidence supports making vitamin D3 and K2 optimization a foundational element of any evidence-based longevity strategy.


